Over the last few years, there has been a lot of buzz about a procedure abbreviated RLE or Refractive Lens Exchange. As an eye surgeon at Las Vegas Eye Institute, I commonly get asked about this procedure and who the procedure is right for. Refractive Lens exchange is where the natural lens of the eye is removed and a new synthetic lens is put in its place. The procedure is actually performed in the exact same fashion as cataract surgery. Like cataract surgery, it is a procedure that can correct nearsightedness, farsightedness, and astigmatism. It is also a treatment for presbyopia which is the natural decline in near visual function as we age.
When do you consider refractive lens exchange and why?
In my practice, I tend to focus this procedure on people who are farsighted. Farsightedness is a confusing term because people who are “farsighted” can see well at a distance only when they are young and their natural lens can overcome the condition. As a farsighted person ages, they begin to have difficulty with near tasks first and later have difficulty with both near and far tasks. A farsighted eye is a short eye that doesn’t have enough power to focus the image onto the retina. In the following image, you can see that the image is focusing behind the retina.
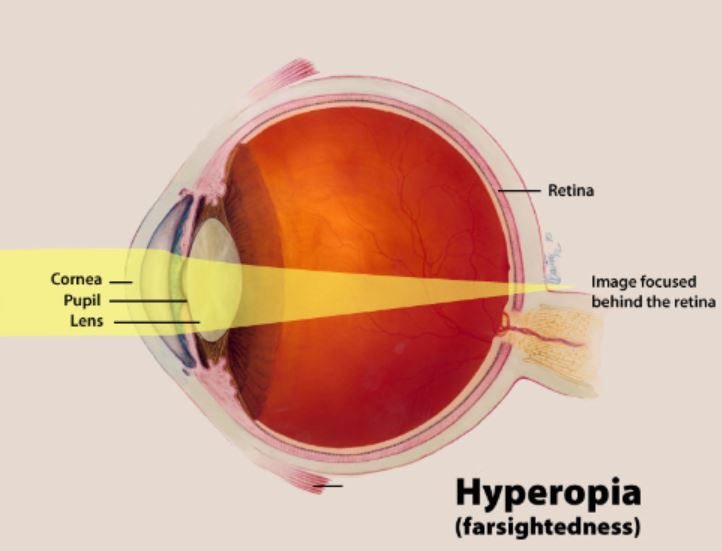
When we are young our natural lens can change its shape to increase power and get the image into focus on the retina. As we age the lens loses it pliability and can no longer change shape enough to get the image in focus on the retina.
Now that we understand farsightedness it may be easy to guess what a surgeon like me does to correct the problem… I increase the power of the lens in the eye. Refractive lens exchange is great for this because we have a variety of lens powers at our disposal and we can correct high levels of farsightedness and still give very good visual quality. If you read our post on LASIK you will find that LASIK can also correct farsightedness but the issue with LASIK is that while the visual quality is good it begins to decline in quality once we correct past approximately 3 diopters of power in farsighted treatments (for nearsighted this is more like 8 diopters). So if a person is farsighted by 5 Diopters their very best option tends to be RLE or refractive Lens exchange as LASIK cannot compete with the optical quality of refractive lens exchange. Even at an advanced practice like Las Vegas Eye Institute where we use customized wavefront-guided iDesign treatments, RLE is still superior for high corrections of farsightedness.
What type of lens should I have put in my eye during refractive lens exchange?
Once we remove a lens during refractive lens exchange we have to replace the power of the lens. This can be done with a conventional monofocal, toric, extended depth of focus or multifocal intraocular lens. If we determine during your evaluation that you don’t have any significant astigmatism a monofocal lens can be a perfect choice and lower your expense as there is no additional cost beyond the cost of the surgery itself. A monofocal lens is usually placed in monovision format for RLE because with this you can see well at distance with your dominant eye and see well at near with your non-dominant eye. To do monovision treatments your surgeon simply needs to increase the power of the lens in the non-dominant eye to give you increased power to see up close. If a patient has significant astigmatism then they may need to opt for a lens that can correct astigmatism, these lenses are referred to as toric lenses. Finally, in 2019 we have the option of extended depth of focus or multifocal intraocular lenses that allow people to see at a distance and near. An extended depth of focus lens allows good computer vision (what ophthalmologists refer to as intermediate vision) while a multifocal lens can allow excellent near vision for finer tasks like reading a book or the newspaper. Both extended depth of focus and multifocal lenses do have a drawback in night driving. Right after their placement people will notice some level of haloes around lights. Fortunately, most of my patients describe it as mild and it does tend to diminish over the first several months after placement.
I am 50 years old and nearsighted. Why did you tell me that RLE isn’t a good idea?
As a refractive surgeon when I encounter patients who are nearsighted I am much more inclined to offer LASIK over RLE for several reasons. The first reason is that LASIK is excellent for nearsightedness. With wavefront-guided treatments on the iDesign platform, we can get outstanding visual outcomes with up to 8 diopters of nearsightedness and correct astigmatism at the same time. Also, we can easily do monovision treatments with LASIK and its even easier in 2019 as the iDesign platform is now the only FDA approved LASER for monovision. This means that we can still offer excellent custom treatments and leave one eye for near. All other FDA approved lasers can only perform wavefront optimized or conventional treatments instead of treating the unique wavefront features of your eye when performing the treatment on the near eye. Lastly, and the most important reason why I don’t perform RLE on nearsighted people is that it is not as safe. Studies have consistently shown that performing cataract surgery (essentially the same procedure as RLE) on myopic patients around the age of 50 leads to a higher rate or retinal detachments after the procedure. If I can give someone an excellent result with a time tested and safe procedure then I will choose that route every time.
What else besides iDesign monovision LASIK is new this year?
In the field of refractive lens exchange, we are eagerly anticipating the arrival of new trifocal intraocular lenses that can allow vision at distance, intermediate, and near vision. The US company Alcon has launched such a lens in Europe. This lens is called the Acrysof IQ Panoptix. We can never be sure when FDA approvals will come but we are expecting this lens to receive FDA approval this year, which should make for an even more exciting time in RLE and cataract surgery.